

INTRODUCTION:
With the advent of newer treatment options for patients with acute leukemia and myeloma, therapies are increasingly safely administered on an outpatient basis. We hypothesized increasing utilization of outpatient options would result in decreased hospitalizations for chemotherapy, albeit with increased hospitalization charges. We interrogated chemotherapy utilization amongst adult inpatients with these malignancies using the National Inpatient Sample (NIS).
METHODS:
The NIS is a database providing information on all inpatient hospitalizations in the United States (US), including primary and secondary diagnoses, procedures, length of stay, and disposition. Approximately 20% of admissions are tracked, and weighted estimates are provided regarding the total number of hospitalizations in the US.
Using the NIS, we tracked chemotherapy admissions for patients with the following hematological malignancies: acute myeloid leukemia (AML), acute lymphoid leukemia (ALL) and multiple myeloma (MM). Admissions for hematopoietic stem cell transplants were excluded from our analysis, and only patients aged 18 or greater were included in our analysis. Procedural International Classification of Disease (ICD) 9 and 10 codes were used to gain insight into trends of hospitalizations, elective versus urgent status, costs and length of stay for each indication. Time frame 2002-2017 was chosen as this was the most recent year for which NIS data is available. Inflation adjustments for charges were calculated based on US Department of Labor statistics.
RESULTS:
For MM, there were a total of 54,357 admissions for chemotherapy from 2002-2017. Amongst these admissions, 37,517 were elective, and 16,670 were non-elective, with the remainder lacking data on elective status.
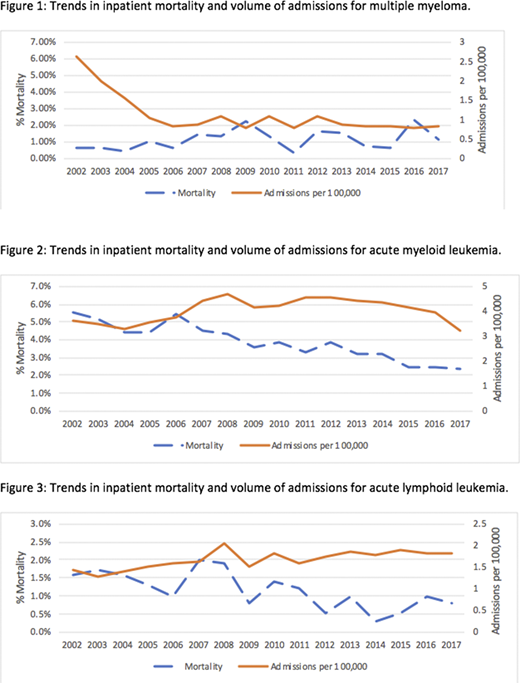
Figure 1 highlights trends in admissions for MM, with a significant decrease noted in the overall volume (7,547 in 2002 to 2,710 in 2014 (p=0.003)). Mortality rates for MM chemotherapy admissions, also highlighted in Figure 1, did not change significantly from 2002 to 2017 (p=0.15). Mean length of stay for chemotherapy hospitalizations increased from 4.67 days in 2002 to 6.47 days in 2017 (p<0.0001). Mean inflation-adjusted hospitalization charges increased from $20,865 in 2002 to $79,161 in 2017 (p<0.0001).
For AML, we noted 198,288 admissions for chemotherapy from 2002-2017 of which 127,277 were considered elective, and 70,566 non-elective, with the remainder lacking data on elective status.
Figure 2 highlights trends in AML admissions with a decreased volume of admissions noted from 2011 onwards after an initial increase from 2005-2008. There was a total of 14,214 admissions in 2011 compared to 10,515 in 2017 (p=0.004) There was a decrease in inpatient mortality rates from 5.5% in 2002 to 2.4% in 2017 (p<0.0001). Mean length of stay was consistent during this time period from 13.35 days in 2002 to 13.34 days in 2017 (p=0.15). Mean inflation-adjusted hospitalization charges increased from $83,904 in 2002 to $133,295 in 2017 (p<0.001).
There was a total of 82,730 admissions for chemotherapy from 2002-2017 for ALL. Amongst these admissions, 54,565 were elective and 27,963 were non-elective, with the remainder lacking data on elective status.
Figure 3 highlights trends in admissions, with an increase in number of admissions from 4,092 in 2002 to 5,960 in 2017 (p=0.86). There was a decrease in the inpatient mortality rate from 0.8% in 2002 to 0.4% in 2017 (p=0.0007). Mean length of stay stayed consistent at 7.70 days in 2002 to 7.62 days in 2017 (p=0.06). Mean inflation-adjusted hospitalization charges increased from $49,283 in 2002 to $94,787 in 2017 (p<0.0001).
CONCLUSIONS:
There has been a steady decline in the number of admissions for inpatient chemotherapy for patients with multiple myeloma and acute myeloid leukemia over time, owing to advances in therapies delivered safely and efficaciously as an outpatient. There has also been a steady decline in inpatient mortality for chemotherapy for acute myeloid and acute lymphoid leukemia, in part due to advances in supportive care. However, the inpatient mortality rate for myeloma has not decreased, likely due to sicker patients preferentially needing admission for inpatient chemotherapy. Inflation-adjusted hospitalization charges have gone up dramatically and further work is needed to elucidate factors driving these costs, and how to mitigate them.
Ganguly:Kadmon: Other: Ad Board; Settle Genetics: Speakers Bureau; KITE Pharma: Speakers Bureau. McGuirk:Astellas: Research Funding; Novartis: Research Funding; Allo Vir: Consultancy, Honoraria, Research Funding; Juno Therapeutics: Consultancy, Honoraria, Research Funding; Kite Pharmaceuticals: Consultancy, Honoraria, Research Funding, Speakers Bureau; Pluristem Ltd: Research Funding; Gamida Cell: Research Funding; Bellicum Pharmaceutical: Research Funding; Fresenius Biotech: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal